
Retatrutide: The Triple Agonist Changing How Clinicians Think About Obesity Medicine
Retatrutide: The Triple Agonist Changing How Clinicians Think About Obesity Medicine
For years, obesity was reduced down to one message: eat less and move more. Meanwhile, clinicians continued watching patients struggle with:
insulin resistance
food cravings
weight regain
inflammation
fatigue
metabolic dysfunction
binge eating patterns
and loss of satiety control
Many patients were blamed for problems deeply connected to biology, signaling, hormones, metabolism, and the brain. That is one reason medications like Semaglutide and Tirzepatide changed medicine so quickly. They forced healthcare professionals to look deeper at metabolic disease, not just body weight. And now a newer medication called Retatrutide is pushing that discussion even further.
What Is Retatrutide?
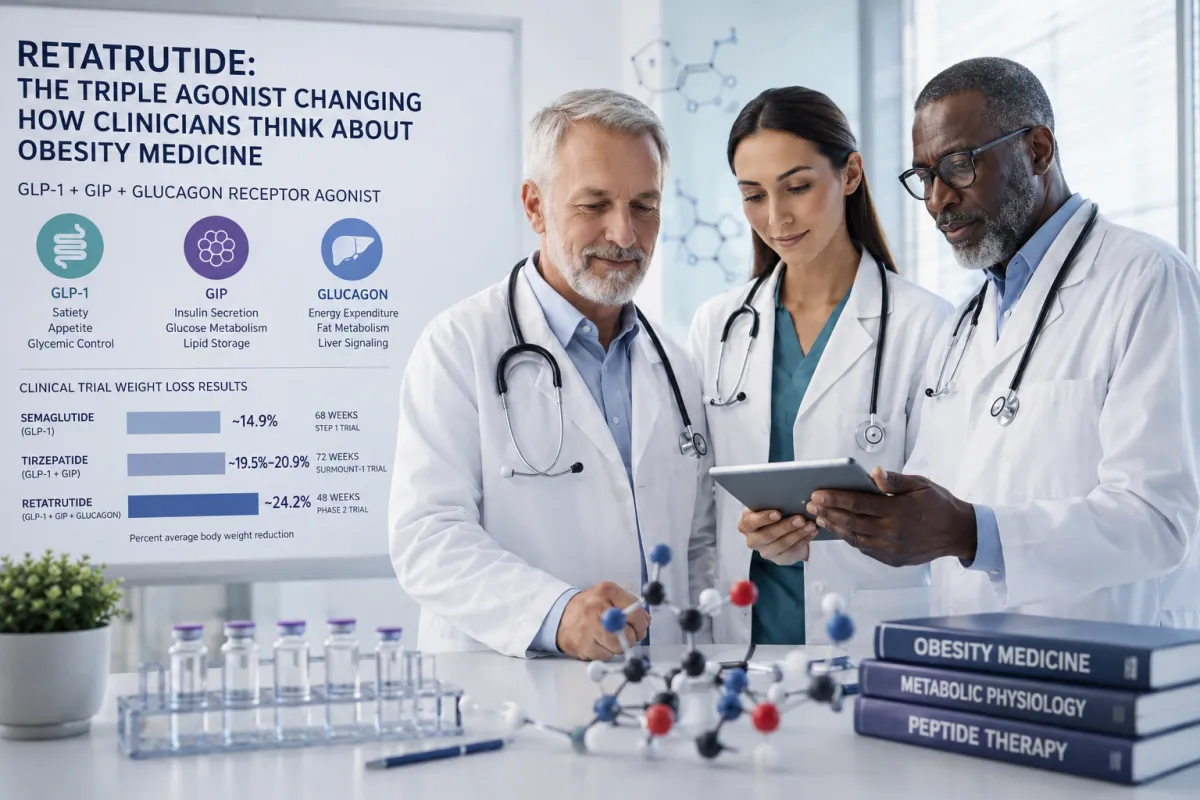
Retatrutide is an investigational peptide being developed for obesity and metabolic disease. What makes it different is that it works through three separate receptors:
GLP-1
GIP
Glucagon
That is why many clinicians refer to it as a triple agonist. Semaglutide mainly works through GLP-1. Tirzepatide works through GLP-1 and GIP. Retatrutide adds a third target: the glucagon receptor. That changes the entire metabolic game.
Why Retatrutide Is Different From Earlier GLP-1 Medications
Most healthcare professionals already understand the basic role of GLP-1 medications. They slow gastric emptying, improve satiety signaling, reduce appetite, and help improve blood sugar regulation. That alone changed obesity dramatically because clinicians finally started seeing how strongly biology influences hunger, eating behavior, and metabolic function.
Then Tirzepatide entered the picture by targeting both GLP-1 and GIP receptors together. That pushed the field further and produced greater weight reduction than earlier GLP-1 medications alone. However, Retatrutide changes everything and takes this one step further by also targeting the glucagon receptor.
Most people were taught to associate glucagon primarily with raising blood sugar. While that is true, glucagon also plays a major role in energy expenditure, fat metabolism, liver signaling, and fuel utilization. Researchers are now looking much deeper at how glucagon signaling may influence metabolic regulation when balanced alongside GLP-1 and GIP activity.
That combination may be part of why Retatrutide produced such significant body weight reduction in clinical trials. This is no longer just about appetite suppression. Researchers are now looking at obesity through a much broader metabolic lens involving energy balance, insulin sensitivity, satiety regulation, body composition, and how the brain and body communicate around fuel usage.
Why Retatrutide Is Getting So Much Attention
One of the biggest reasons Retatrutide stands out is the amount of weight reduction seen in early clinical trials. Semaglutide 2.4 mg produced about 14.9% average body weight reduction at 68 weeks in the STEP 1 trial. Tirzepatide produced about 19.5% to 20.9% average body weight reduction at 72 weeks in the SURMOUNT-1 trial. In a phase 2 trial published in The New England Journal of Medicine, Retatrutide produced up to 24.2% average body weight reduction at 48 weeks in adults with obesity.
These trials were not identical, so the numbers should not be compared as if they came from the same study. However, they do help clinicians understand why Retatrutide is getting so much attention. Semaglutide targets GLP-1. Tirzepatide targets GLP-1 and GIP. Retatrutide targets GLP-1, GIP, and Glucagon.
That is what makes Retatrutide different. The discussion is no longer only about appetite suppression. Researchers are now looking much deeper at energy balance, insulin sensitivity, satiety signaling, liver metabolism, and how the body uses fuel.
Obesity is not simply a lack of discipline. Clinicians see patients every day who are fighting much more than willpower, including:
hunger signaling
insulin resistance
reward-driven eating
poor satiety signaling
metabolic adaptation
inflammation
and dysregulated energy balance
That is why these medications are changing how healthcare professionals think about obesity medicine overall.
Why Obesity Is More Complex Than Willpower
One of the most important things GLP-1 medications expose is how many patients live with constant food noise. Constant thoughts about food, persistent cravings, hunger, and reward-seeking tied to eating can become exhausting for patients who are trying to regain control of their health.
Many patients describe finally feeling “quiet” in their brain for the first time after starting GLP-1-based medications. This is one reason clinicians are starting to look more closely at the brain’s role in obesity, craving, reward behavior, and metabolic dysfunction.
Research is also exploring whether GLP-1 receptor agonists may have a role beyond food cravings, including alcohol use disorder and substance use disorders. Early studies suggest these medications may influence reward signaling in the brain, including dopamine-related circuits involved in craving and reinforcement. In a small randomized clinical trial, semaglutide reduced some measures of alcohol consumption and significantly reduced weekly alcohol craving compared with placebo. More research is still needed before these medications can be viewed as addiction treatments, but the signal is important.
People are not weak for struggling against biology. The brain, gut, hormones, inflammation, insulin signaling, dopamine response, and metabolic regulation all play a role in eating behavior, cravings, and reward-seeking behavior. Retatrutide may push clinicians to look even deeper at those connections.
Retatrutide Is Bigger Than Weight Loss
Retatrutide is not interesting simply because of body weight reduction.
It is interesting because it may help healthcare professionals better understand:
- obesity
- metabolic disease
- satiety signaling
- reward behavior
- insulin resistance
- inflammation
- fatty liver disease
- cardiovascular risk
- and energy regulation
That is a much bigger discussion than aesthetics. Healthcare professionals are now watching metabolic medicine shift in real time. Medicine needed this shift because patients have spent years being blamed for biology they often did not fully control.
Why Clinicians Need To Understand These Medications
Healthcare professionals do not need to memorize protocols to understand peptides like Retatrutide. They need to understand physiology. They need to understand why satiety signaling matters, how insulin resistance changes metabolism, why inflammation affects metabolic health, how reward signaling influences eating behavior, what happens when multiple receptors are targeted at once, and why obesity is far more complex than calories alone.
That is where peptide education becomes important. Healthcare professionals need a deeper understanding of the body systems they are treating every day. When clinicians understand medications like Retatrutide from a physiological and clinical perspective, they are better prepared to educate patients, set realistic expectations, and think critically through what may or may not make sense in patient care.
The Future Of Metabolic Medicine Is Already Changing
Retatrutide is still investigational. Long-term safety data is still needed, along with more research, and more clinical experience. However, medicine is entering a completely different era of metabolic treatment.
Obesity is increasingly being understood through:
- signaling
- hormones
- neurobiology
- inflammation
- metabolism
- and energy regulation
That shift will change healthcare for decades. Clinicians who understand these peptides beyond surface-level weight loss discussions will be far better prepared to care for the patients sitting in front of them.
About The Author
Lauren Supra, RN, BC-FMP is the founder of Advera Care and creator of Peptide Therapy in Clinical Practice, an accredited continuing medical education program designed to help licensed healthcare professionals better understand peptide therapy, physiology, and responsible clinical integration.
References
Drucker, D. J. (2022). GLP-1 physiology informs the pharmacotherapy of obesity. Molecular Metabolism, 57, 101351. https://doi.org/10.1016/j.molmet.2021.101351
Jastreboff, A. M., Kaplan, L. M., Frías, J. P., Wu, Q., Du, Y., Gurbuz, S., Coskun, T., Haupt, A., & Milicevic, Z. (2023). Triple-hormone-receptor agonist retatrutide for obesity — A phase 2 trial. The New England Journal of Medicine, 389(6), 514–526. https://doi.org/10.1056/NEJMoa2301972
Müller, T. D., Finan, B., Clemmensen, C., DiMarchi, R. D., & Tschöp, M. H. (2017). The new biology and pharmacology of glucagon. Physiological Reviews, 97(2), 721–766. https://doi.org/10.1152/physrev.00025.2016
Sanyal, A. J., Kaplan, L. M., Frias, J. P., Bchir, M. B., Cheng, A., Pham, T., Pavo, I., Chen, S., Gurbuz,S., Haupt, A., & Jastreboff, A. M. (2024). Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease: A randomized phase 2 trial. Nature Medicine, 30, 2037–2046. https://doi.org/10.1038/s41591-024-03018-2
Wharton, S., Lau, D. C. W., Vallis, M., Sharma, A. M., Biertho, L., Campbell-Scherer, D., Adamo, K., Alberga, A., Bell, R., Boulé, N., Boyling, E., Brown, J., Calam, B., Clarke, C., Crowshoe, L., Divalentino, D., Forhan, M., Freedhoff, Y., Gagner, M., … Wicklum, S. (2020). Obesity in adults: A clinical practice guideline. Canadian Medical Association Journal, 192(31), E875–E891. https://doi.org/10.1503/cmaj.191707
Aronne, L. J., Sattar, N., Horn, D. B., Bays, H. E., Wharton, S., Lin, W.-Y., Ahmad, N. N., Zhang, S., Liao, R., Bunck, M. C., Jouravskaya, I., Murphy, M. A., & SURMOUNT-1 Investigators. (2024). Continued treatment with tirzepatide for maintenance of weight reduction in adults with obesity: The SURMOUNT-4 randomized clinical trial. JAMA, 331(1), 38–48. https://doi.org/10.1001/jama.2023.24945
Wilding, J. P. H., Batterham, R. L., Calanna, S., Davies, M., Van Gaal, L. F., Lingvay, I., McGowan, B. M., Rosenstock, J., Tran, M. T. D., Wadden, T. A., Wharton, S., Yokote, K., Zeuthen, N., & Kushner, R. F. (2021). Once-weekly semaglutide in adults with overweight or obesity. The New England Journal of Medicine, 384(11), 989–1002. https://doi.org/10.1056/NEJMoa2032183
Hendershot, C. S., Bremmer, M. P., Paladino, N. J., et al. (2025). Once-weekly semaglutide in adults with alcohol use disorder: A randomized clinical trial. JAMA Psychiatry. https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2829811
Klausen, M. K., Thomsen, M., Wortwein, G., & Fink-Jensen, A. (2022). The role of glucagon-like peptide 1 (GLP-1) in addictive disorders. British Journal of Pharmacology, 179(4), 625–641. https://doi.org/10.1111/bph.15677


